


Governing the Global Body: A Sociological Reading of the Amended International Health Regulations
(Relevant for Sociology Paper 2: Population Dynamics)
Governing the Global BodyThe recent entry into force of the amended International Health Regulations (IHR) is typically framed as a milestone in technical global health policy. However, a sociological lens reveals a far more profound story: the IHR represents a monumental project in global social ordering, a fascinating case study of how societies attempt to manage risk, negotiate sovereignty, and confront the deep-seated inequalities that shape life and death itself. This is not merely a health document; it is a blueprint for a new form of transnational social contract in an age of perpetual pandemic threat. From Quarantine to Biopower: The Historical Arc of Global Health Governance
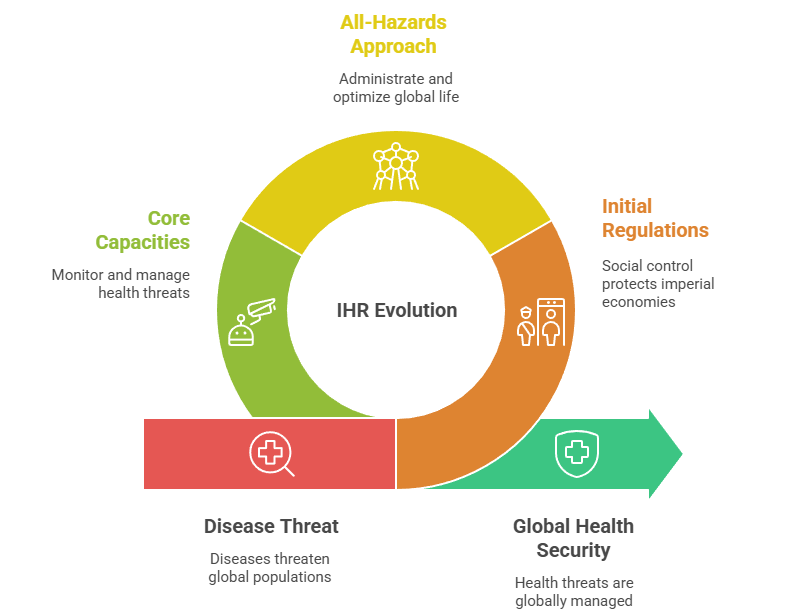
The genesis of the IHR at the 1851 International Sanitary Conference, convened to combat cholera along European trade routes, is deeply revealing. This was not primarily about altruism; it was about the sociology of borders and commerce. The initial regulations were a tool of social control designed to protect imperial economies and European populations from the diseases of the “Orient.” The focus was on cordons sanitaires and quarantine—a defensive, exclusionary model of public health. The evolution of the IHR—from the narrow focus on three diseases in 1969 to the all-hazards approach of 2005—traces a shift in the nature of global power, as articulated by Michel Foucault. We see a move from a “sovereign power” that simply prohibits and isolates, to a “biopower” that seeks to administrate and optimize the life of the population at a global scale. The IHR 2005, with its demand for 24-hour notification and the development of national “core capacities,” represents an ambitious project of global biopower. It aims to make health threats globally legible, monitorable, and manageable, transforming nation-states into nodes in a worldwide surveillance and response network. The Pandemic Emergency: Codifying a Global Social FactThe introduction of the new ‘Pandemic Emergency’ category in the 2024 amendments is a direct sociological response to the COVID-19 experience. A pandemic is not just a biological event; it is a total social fact, a term coined by Marcel Mauss to describe phenomena that simultaneously engage the economic, legal, political, and religious institutions of a society. The new classification acknowledges this reality. By defining a Pandemic Emergency as an event that causes “major social and economic disruption,” the IHR formally recognizes that modern health crises are crises of the entire social order. This legal categorization acts to trigger a pre-defined set of international social responses, attempting to bring order to the chaos that inevitably accompanies a breakdown in supply chains, labour markets, and social trust. National IHR Authorities: The State as a Manager of Biological RiskThe mandate for each country to establish a National IHR Authority is a crucial step in institutionalizing this global biopower. This moves the IHR beyond the health ministry, requiring coordination across transport, trade, and security. This can be seen as the creation of what Ulrich Beck would call a “risk management” apparatus at the state level. In a “World Risk Society,” Beck argues, the primary conflicts are no longer over the distribution of wealth, but over the distribution of risks—like pandemics—which are unequally distributed but ultimately borderless. The National IHR Authority is the institutional embodiment of the state’s role in managing this new class of global biological risk. For India, this means creating a permanent bureaucratic structure whose mandate is to constantly prepare for a future catastrophe, a fascinating example of the state pre-emptively organizing itself around a potential, rather than a present, social problem. Equity as a Structural Challenge: Beyond Charity to Justice
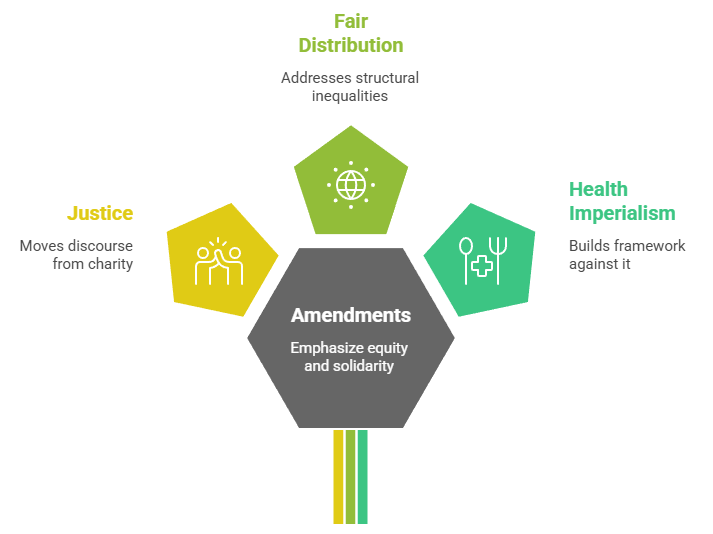
The amendments’ strong emphasis on “equity and solidarity” in access to medical countermeasures is a direct admission of the catastrophic failures of vaccine nationalism during COVID-19. Sociologically, this moves the discourse from charity to justice. The “fair distribution” clauses are an attempt to address what Thomas Piketty and others highlight as the deepening structural inequalities between nations. The pandemic laid bare a global class system, where wealthier nations could hoard vaccines while low- and middle-income countries waited. The IHR amendments represent a fragile consensus that this is not only morally indefensible but also epidemiologically irrational. By placing equity at its core, the IHR is attempting to build a normative framework against “health imperialism,” though its success remains entirely dependent on the political will of powerful states to cede advantage. Compliance and the Performance of SovereigntyThe reliance on Joint External Evaluations (JEE) for monitoring reveals the limits of the IHR’s power. The IHR is legally binding, but it lacks a strong enforcement mechanism. Compliance, therefore, becomes a form of “performance,” a concept used in sociology to describe how actors present themselves to a relevant audience. For nation-states, participating in a JEE and publishing reports is a way to perform “responsible sovereignty” and “good global citizenship.” It signals to other nations, international institutions, and global capital that the country is a safe and stable place. This performance enhances a state’s “symbolic capital,” potentially attracting investment and avoiding travel bans during a crisis. The power of the IHR, therefore, lies less in its legal coercion and more in its ability to create a global standard of conduct that states feel compelled to be seen as upholding. Conclusion: A Fragile Blueprint for a Shared FutureThe amended IHR is a remarkable social artifact. It is an imperfect, contested, and politically fraught attempt to construct a system of global solidarity in a world of sovereign, unequal states. It embodies the transition from a public health model based on exclusionary borders to one based on integrated, but often inequitable, interdependence. Ultimately, the sociology of the IHR shows us that the greatest challenges to global health are not viral, but social. They are challenges of trust, equity, and collective action. The amended regulations provide the scaffolding for a more resilient global society, but whether that society emerges will depend on our ability to solve the ancient problems of power and privilege that the pandemic so brutally exposed. The IHR is not just a set of rules for fighting disease; it is a mirror reflecting our capacity for global cooperation in the face of a shared biological destiny. |


To Read more topics, visit: www.triumphias.com/blogs
Read more Blogs:
Universal Immunisation Programme in India: Progress, Challenges, and Sociological Insights
Changing Mode of Production in Indian Agriculture: Desertification and Farming Technology
This sociological reading of the IHR provides a much-needed perspective, showing how global health governance isn’t just about policy, but also about shaping social structures and behaviors. It’s interesting to think about how health regulations are used as tools of biopower and control, especially in the context of pandemics.