
Pandemics: Risks, Impacts, and Mitigation
Relevance: Sociology: Population Dynamics:
(a) Population size, growth, composition and distribution.
(b) Components of population growth: birth, death, migration.
INTRODUCTION

Pandemics are large-scale outbreaks of infectious disease that can greatly increase morbidity and mortality over a wide geographic area and cause significant economic, social, and political disruption. Evidence suggests that the likelihood of pandemics has increased over the past century because of increased global travel and integration, urbanization, changes in land use, and greater exploitation of the natural environment. These trends likely will continue and will intensify. Significant policy attention has focused on the need to identify and limit emerging outbreaks that might lead to pandemics and to expand and sustain investment to build preparedness and health capacity.
The international community has made progress toward preparing for and mitigating the impacts of pandemics. The 2003 severe acute respiratory syndrome (SARS) pandemic and growing concerns about the threat posed by avian influenza led many countries to devise pandemic plans. Delayed reporting of early SARS cases also led the World Health Assembly to update the International Health Regulations (IHR) to compel all World Health Organization member states to meet specific standards for detecting, reporting on, and responding to outbreaks (WHO 2005). The framework put into place by the updated IHR contributed to a more coordinated global response during the 2009 influenza pandemic. International donors also have begun to invest in improving preparedness through refined standards and funding for building health capacity .
Despite these improvements, significant gaps and challenges exist in global pandemic preparedness. Progress toward meeting the IHR has been uneven, and many countries have been unable to meet basic requirements for compliance. Multiple outbreaks, notably the 2014 West Africa Ebola epidemic, have exposed gaps related to the timely detection of disease, availability of basic care, tracing of contacts, quarantine and isolation procedures, and preparedness outside the health sector, including global coordination and response mobilization. These gaps are especially evident in resource-limited settings and have posed challenges during relatively localized epidemics, with dire implications for what may happen during a full-fledged global pandemic.
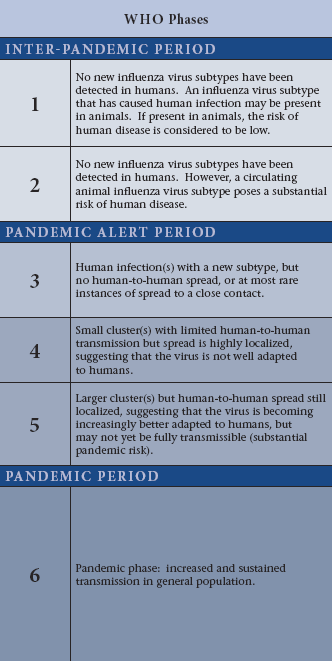
For the purposes of this chapter, an epidemic is defined as “the occurrence in a community or region of cases of an illness . . . clearly in excess of normal expectancy” . A pandemic is defined as “an epidemic occurring over a very wide area, crossing international boundaries, and usually affecting a large number of people” . Pandemics are, therefore, identified by their geographic scale rather than the severity of illness. For example, in contrast to annual seasonal influenza epidemics, pandemic influenza is defined as “when a new influenza virus emerges and spreads around the world, and most people do not have immunity” (WHO 2010).
Endemic diseases are far more common than pandemics and can have significant negative health and economic impacts, especially in low- and middle-income countries (LMICs) with weak health systems. Additionally, given the lack of historical data and extreme uncertainty regarding bioterrorism, this chapter does not specifically consider bioterrorism-related events, although bioterrorism could hypothetically lead to a pandemic.
Risks
- Pandemics have occurred throughout history and appear to be increasing in frequency, particularly because of the increasing emergence of viral disease from animals.
- Pandemic risk is driven by the combined effects of spark risk (where a pandemic is likely to arise) and spread risk (how likely it is to diffuse broadly through human populations).
- Some geographic regions with high spark risk, including Central and West Africa, lag behind the rest of the globe in pandemic preparedness.
- Probabilistic modeling and analytical tools such as exceedance probability (EP) curves are valuable for assessing pandemic risk and estimating the potential burden of pandemics.
- Influenza is the most likely pathogen to cause a severe pandemic. EP analysis indicates that in any given year, a 1 percent probability exists of an influenza pandemic that causes nearly 6 million pneumonia and influenza deaths or more globally.
Impacts
- Pandemics can cause significant, widespread increases in morbidity and mortality and have disproportionately higher mortality impacts on LMICs.
- Pandemics can cause economic damage through multiple channels, including short-term fiscal shocks and longer-term negative shocks to economic growth.
- Individual behavioral changes, such as fear-induced aversion to workplaces and other public gathering places, are a primary cause of negative shocks to economic growth during pandemics.
- Some pandemic mitigation measures can cause significant social and economic disruption.
- In countries with weak institutions and legacies of political instability, pandemics can increase political stresses and tensions. In these contexts, outbreak response measures such as quarantines have sparked violence and tension between states and citizens.
Mitigation
- Pathogens with pandemic potential vary widely in the resources, capacities, and strategies required for mitigation. However, there are also common prerequisites for effective preparedness and response.
- The most cost-effective strategies for increasing pandemic preparedness, especially in resource-constrained settings, consist of investing to strengthen core public health infrastructure, including water and sanitation systems; increasing situational awareness; and rapidly extinguishing sparks that could lead to pandemics.
- Once a pandemic has started, a coordinated response should be implemented focusing on maintenance of situational awareness, public health messaging, reduction of transmission, and care for and treatment of the ill.
- Successful contingency planning and response require surge capacity—the ability to scale up the delivery of health interventions proportionately for the severity of the event, the pathogen, and the population at risk.
- For many poorly prepared countries, surge capacity likely will be delivered by foreign aid providers. This is a tenable strategy during localized outbreaks, but global surge capacity has limits that likely will be reached during a full-scale global pandemic as higher-capacity states focus on their own populations.
- Risk transfer mechanisms, such as risk pooling and sovereign-level catastrophe insurance, provide a viable option for managing pandemic risk.
Consequences of Pandemics
Health Impacts
The direct health impacts of pandemics can be catastrophic. During the Black Death, an estimated 30–50 percent of the European population perished. More recently, the HIV/AIDS pandemic has killed more than 35 million persons since 1981.
Pandemics can disproportionately affect younger, more economically active segments of the population. During influenza pandemics (as opposed to seasonal outbreaks of influenza), the morbidity and mortality age distributions shift to younger populations, because younger people have lower immunity than older people, which significantly increases the years of life lost. Furthermore, many infectious diseases can have chronic effects, which can become more common or widespread in the case of a pandemic. For example, Zika-associated microcephaly has lifelong impacts on health and well-being.
The indirect health impacts of pandemics can increase morbidity and mortality further. Drivers of indirect health impacts include diversion or depletion of resources to provide routine care and decreased access to routine care resulting from an inability to travel, fear, or other factors. Additionally, fear can lead to an upsurge of the “worried well” seeking unnecessary care, further burdening the health care system.
During the 2014 West Africa Ebola epidemic, lack of routine care for malaria, HIV/AIDS, and tuberculosis led to an estimated 10,600 additional deaths in Guinea, Liberia, and Sierra Leone. This indirect death toll nearly equaled the 11,300 deaths directly caused by Ebola in those countries . Additionally, diversion of funds, medical resources, and personnel led to a 30 percent decrease in routine childhood immunization rates in affected countries. During the 2009 influenza pandemic, a greater surge in hospital admissions for influenza and pneumonia was associated with statistically significant increases in deaths attributable to acute myocardial infarction and stroke. However, during a pandemic, distinguishing which deaths are attributable to the pandemic itself and which are merely coincidental may be impossible.
During the 2014 West Africa Ebola epidemic, facilities closures as a result of understaffing and fear of contracting the disease played a large role in lack of access to or avoidance of routine health care. One study of 45 public facilities in Guinea found that the Ebola outbreak led to a 31 percent decrease in outpatient visits for routine maternal and child health services. Among children under age five years, hospitals witnessed a 60 percent decrease in visits for diarrhea and a 58 percent decrease in visits for acute respiratory illness (ARI), while health centers saw a 25 percent decrease in visits for diarrhea and a 23 percent decrease in visits for ARI. In Sierra Leone, visits to public facilities for reproductive health care fell by as much as 40 percent during the outbreak (UNDP 2014).
The availability of health care workers also decreases during a pandemic because of illness, deaths, and fear-driven absenteeism. Viral hemorrhagic fevers such as Ebola take an especially severe toll on health care workers, who face significant exposure to infectious material:
During the first Ebola outbreak in the Democratic Republic of Congo in 1976 (then called Zaire), the Yambuku Mission Hospital—at the epicenter of the outbreak—was closed because 11 out of the 17 staff members had died of the disease (WHO 1978).
During the Kikwit Ebola outbreak in 1995 in the same country, 24 percent of cases occurred among known or possible health care workers.
During the 2014 West Africa Ebola epidemic, health care workers experienced high mortality rates: 8 percent of doctors, nurses, and midwives succumbed to Ebola in Liberia, 7 percent in Sierra Leone, and 1 percent in Guinea.
Even if health care workers do not die, their ability to provide care may be reduced. At the peak of a severe influenza pandemic, up to 40 percent of health care workers might be unable to report for duty because they are ill themselves, need to care for ill family members, need to care for children because of school closures, or are afraid.
For more such notes, Articles, News & Views Join our Telegram Channel.
Click the link below to see the details about the UPSC –Civils courses offered by Triumph IAS. https://triumphias.com/pages-all-courses.php