
The Influenza pandemic of 1918 killed about 5% of India’s population. This article finds that districts most adversely affected by influenza mortality saw a temporary increase in the country’s female labour force participation in 1921, driven in part, by distress labour supply by widows and higher wages. The increase was concentrated in the service sector, and had been reversed by 1931.
The Influenza pandemic of 1918 killed around 50 million people globally. Over 13 million of those who died were in India, close to 5% of the country’s total population (Chandra et al. 2012). The pandemic began in the Bombay region and spread to the north and east. It disproportionately killed individuals of working age (20-45 year olds) and was concentrated in districts that experienced less-than-normal levels of humidity. In recent research, we study the short- and medium-run effects of this major demographic shock on women’s employment (Fenske et al. 2020).
There are several examples from history that document the short-run effect of demographic shocks on women’s labour market behaviour. The Black Death, for example, led to the growth of a labour market for women in North-Western Europe (De Moor and Van Zanden 2010). The World Wars increased women’s labour market participation (Boehnke and Gay 2019, Goldin and Olivetti 2013, Acemoglu et al. 2004). In India, the pandemic led to a shortage of labour and created a situation in which women could potentially participate in the labour force and substitute for men in activities previously performed by men. This could have generated short-run and longer run increases in female labour force participation (FLFP) during the 1920s and 1930s. The impact of this demographic shock on female labour supply could persist if women’s working behaviour was transmitted to subsequent generations. By contrast, it could be short-lived if norms against women’s work are strong.
Female labour force participation in India
Today India has one of the lowest low levels of participation of women in economic activity outside the home. A recent literature (for example, Fletcher et al. 2017) on FLFP has highlighted a declining trend, despite rising incomes and greater education of women. Early marriage, social conservatism, and limited participation of women in certain economic activities are among the explanations that have been cited. The influenza epidemic provides a natural experiment with which to look at the effect of a demographic shock on FLFP in India, where cultural norms deter women’s participation in the labour market.
The rate of FLFP in 1901, averaged across districts, was 31%, higher than the 21% reported by the World Development Indicators for 2019. This is not surprising: women’s participation in economic activity is higher in agricultural societies at low levels of income. In 1911, 73% of women workers were in agriculture and related activities; 11% in industry, mining, and construction; 12% in trade, transport, and other services; and 4% in what the census called “insufficiently described occupations.” The latter, which included small jobs in agriculture, construction, and services, the share of women workers could be as high as 40%. Roy (2005) identifies gender segmentation in the colonial labour market. The work done by women was concentrated in specific industries and services, including bidi rolling, hand spinning, basket weaving, grain processing by hand, and stone cutting. Some industries rarely hired women. These included metal working, chemicals, and printing. Some industries employed both men and women, though specific tasks were largely segregated by gender, as in mining, cotton textiles, and quarries.
How the influenza pandemic impacted women’s work participation
We use district-level influenza mortality data for India from the Sanitary Reports of 1918 and 1919 that cover the districts under British rule. We combine these with historical data on FLFP from the decadal censuses of 1901 through 1931, to create a district-level panel dataset on women’s labour market participation. We define participation rate as number of main workers by gender divided by population, to allow for participation rate to include child workers and older workers. We consider both aggregate participation for women and participation in the specific sectors of agriculture, industry, and services. We estimate the short- and medium-run effects of the pandemic by adopting an ‘event study’ method that compares the change in women’s employment in districts that were exposed to different levels of influenza mortality before and after the influenza pandemic. The following maps show women’s participation rate in the labour market in 1911, the district-level variation in mortality, and the change in participation between 1911 and 1921.
Figure 1. Female labour force participation in India, 1911
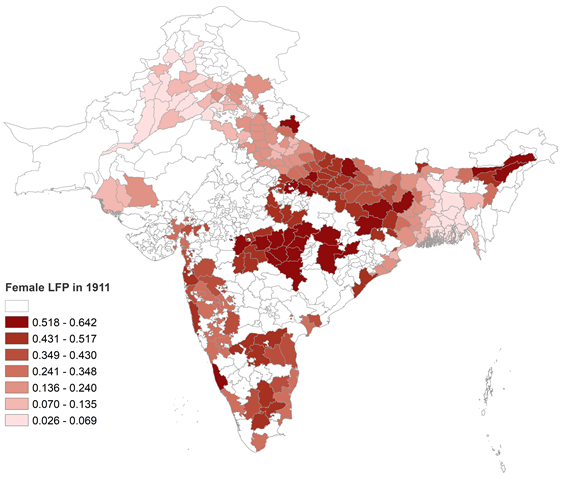 Source: Decadal census.
Source: Decadal census.
Figure 2. District-level variation in influenza mortality
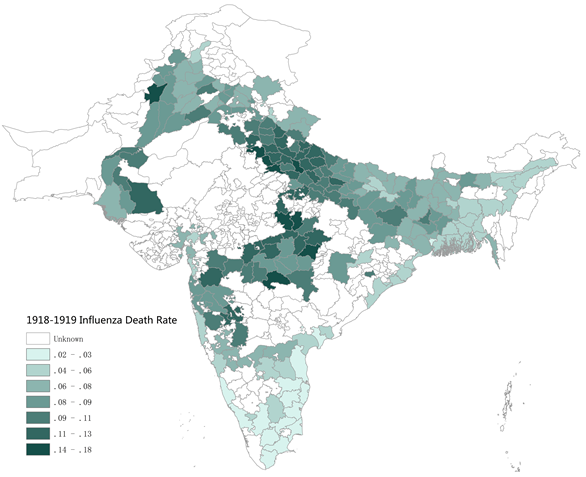 Source: Sanitary reports (1918, 1919).
Source: Sanitary reports (1918, 1919).
Figure 3. Changes in female labour force participation, 1911-1921
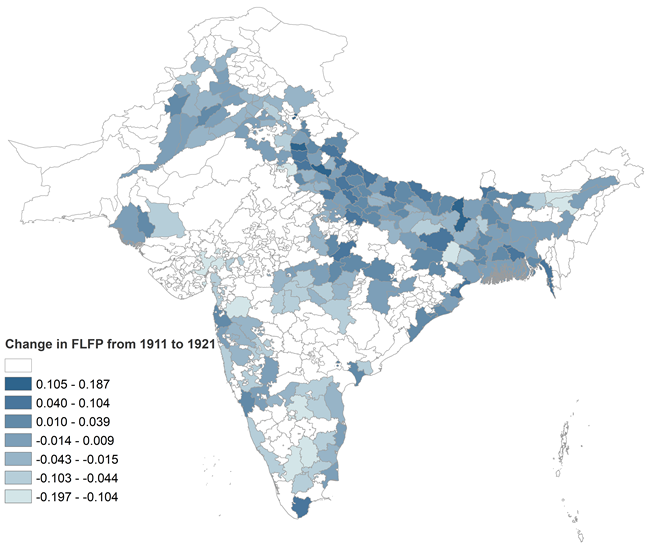
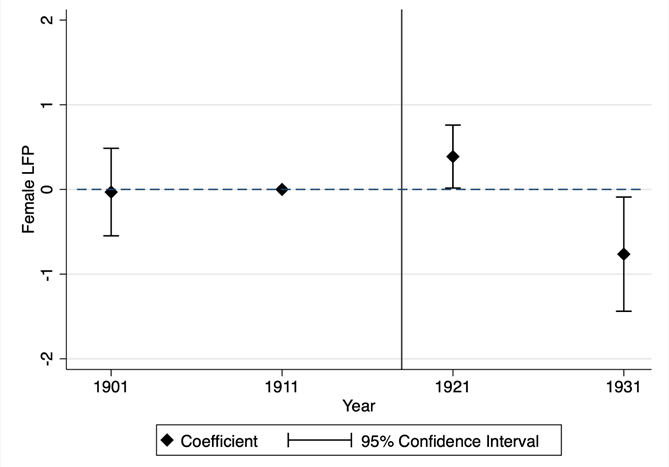
We find that women’s labour force participation increased in districts that experienced greater mortality during the pandemic. The mortality shock experienced by a typical district led FLFP to be 2.3 percentage points higher in 1921 than it would have been otherwise. It increased only in services and only in the 1921 census. The rise was followed by a decline in 1931. In relation to other studies of demographic shocks and FLFP, the response was comparable in magnitude. For France, moving from the 25th to the 75th percentile of the male death rate during the First World War increased FLFP by 3.5 percentage points during the interwar period (Boehnke and Gay 2019).
Figure 4. Influenza pandemic and changes in female labour force participation
We test two potential mechanisms that could potentially drive the short-run results. On the one hand, women might have needed to enter the labour market in order to mitigate the economic shock due to the death of their husbands or other male relatives during the pandemic. On the other hand, the general shortage of labour could have driven up wages and induced more women to join the labour force. Reduced population may, however, have also reduced demand, lessening the availability of jobs. We show that the share of women who were widowed rose in districts more greatly affected by the pandemic and that districts with greater shares of widows saw an increase in FLFP, both in the aggregate and in services. We find no effect on agriculture or industry. We also find evidence of increased participation in districts with lower population density, suggesting that female participation in services grew when labour was scarcer. However, while both these channels can help explain our results, they do not fully mediate them. We find no evidence of a response of male labour force participation to the influenza pandemic, confirming that the changes in women’s labour market participation were not part of a more generalised increase in labour force participation in response to higher wages.
Finally, to evaluate whether the impact of the influenza pandemic was greatest in districts where there was a greater pent-up supply of underutilised female labour, we divide the sample into districts with above and below median levels of FLFP in 1901, the first year in our data. We find that the increase was driven by districts with initially greater levels of FLFP. Rather than the influenza pandemic working to break the constraints imposed by social norms on FLFP, these results suggest that the response itself was constrained by the presence of these norms, or by the prevalence of activities in which women did not work.
Courtesy : James Fenske (University of Warwick) , Bishnupriya Gupta (University of Warwick) , Song Yuan (University of Warwick).